
As a
preamble to what will subsequently be opined in this blog, I want to
strongly underline the fact that the few days leading up to my daughter's
birthday usually have me thinking back to my incompetent Jokewood doctor, Dr. L*b*m*f*. Now, as fate would have it, I was already 2 weeks
post-dates on January 8th, 1980 and had gained 50% of my very early pregnancy
weight of just 90 lbs. Here is part of the problem: Dr. L. had forgotten how
tiny I naturally was and never suspected that I was carrying a 10 lb. baby.
This was a bona fide case of cephalo-pelvic disproportion and my bungling doctor
was at a total loss. I would learn years later of his battle with alcohol and suspect that he was likely 'hung over' the
night I went into hard labor. The truth of the matter is, however, that my
first pangs of labor actually began on a Saturday and my daughter did not
arrive [mid-forceps
extraction style, no less!] until the following Tuesday.
Yet my doctor simply failed to read the writing on the proverbial wall.
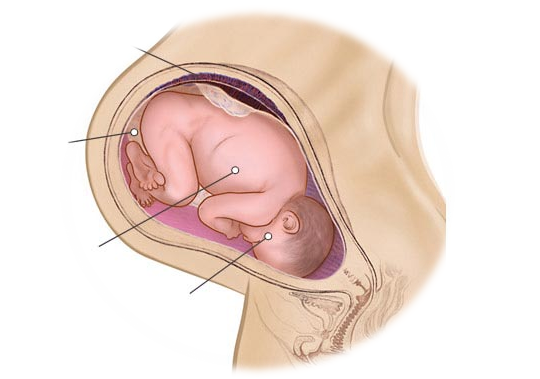
THE DREADED 'SUNNY SIDE UP' FETAL PRESENTATION
The worst
possible thing that can happen in a 'posterior occiput' labor is when the water
breaks (or is intentionally
broken by medical personnel to try to hasten labor) and uterine contractions are both suddenly and rather
dramatically enhanced; the baby's head automatically descends a little bit
more, merely worsening the whole situation. Now, in order for the occipital
component of the fetal skull to become anterior (as it must be for a normal delivery to take
place), it is necessary for the infant's
head to go through an extended rotation of approximately 180 degrees. (Normal
rotation requires only up to a 90 degree turn). Moreover, if the baby's head
descends too deeply into a comparatively undersized pelvis before any such rotation
is effectively completed, the risk of a 'deep transverse arrest' increases,
greatly reducing the chances for a successful vaginal delivery.
What's more problematic
is that if the nurses or doctor(s) do not adequately diagnose this unfavorable
fetal head position until far too late within labor, the only recourse may be to
offer a para-cervical block or epidural anesthesia. You see, it is now virtually
impossible for the mother to relax enough and permit the deep muscles of
the pelvic floor to fully 'loosen up' and consequently allow the baby to sufficiently
turn; and this is the ONLY way for a successful delivery. And nothing in
this world can prepare a mother for the severely excruciating and unremitting
pain that accompanies labor when the baby is in an occiput posterior position.

However, the main tip-off of this potential situation is that the labor typically
begins with short, painful, but 'irregular' contractions. This constitutes a
warning sign of cephalo-pelvic disproportion; in the past, many women died from
this unfortunate circumstance! Yet, this key sign is often shrugged off by
incompetent medical personnel as "false labor."

In reality, it's that
this type of labor is basically just not productive enough: the rather ill-fitting
posterior head is not properly applied to the maternal cervix, even while the
mother IS experiencing great discomfort! She is often sent home to wait for
"real labor" to begin but is unable to sleep and often unable to eat,
as well (because of the pain), sometimes even for several days. So, adding
to the stress of a painful back labor, we begin with a mother who is already exhausted!
I have heard women describe the pain as "it felt as though someone were
literally sawing the back of my body in half" or, "I couldn't even
tell when I was having contractions because my pain was so excruciating!"
All attempts to ease the pain will have little effect [without medication] and the labor is a very long and hard one.

SAID BY A MIDWIFE: "I would love
to see this picture changed. As a midwife, it is my goal to do everything that
I can to help the mother to achieve an optimum birth outcome, to use my skills
to alleviate unnecessary pain and suffering and to help a new family begin in
safety, peace and joy".

Yes,
it's a land 'down-under' where women go and make "thunder"
















